
Fear of heights can be overcome using virtual reality to simulate dizzying experiences such as being perched on the edge of a 10th-floor balcony, a study has shown.
Psychiatrists in Oxford tested the therapy on 100 volunteers with a serious height phobia who responded to adverts on local radio.
They were split into two groups, one of which underwent six 30-minute virtual reality (VR) sessions over a period of two weeks.
Patients wore VR headsets that immersed them in a virtual world where, guided by an avatar “coach”, they were encouraged to face their fears.


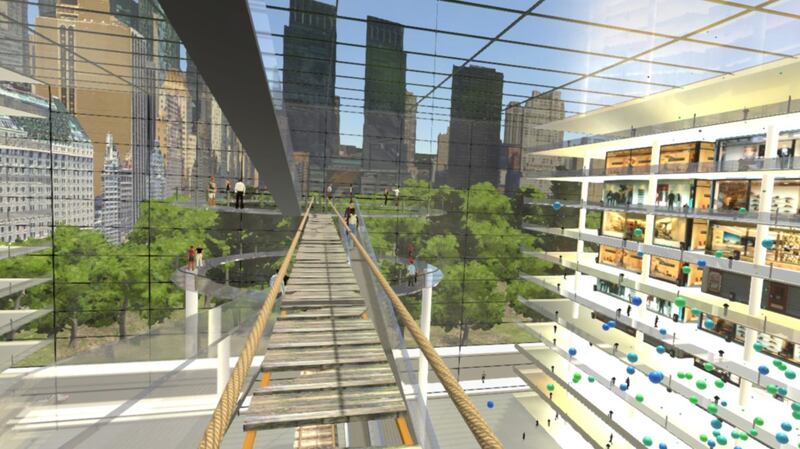
Within the simulation, each participant was taken to a 10-storey office block with a yawning atrium.
There, they engaged in activities designed to be both entertaining and increasingly terror-defying.
Examples included crossing a rickety walkway, stepping out on a platform with no safety barriers, rescuing a cat from a tree, and playing a xylophone on the edge of a balcony.

Finally, they were given the opportunity to ride a virtual whale around the atrium space.
Professor Daniel Freeman, from Oxford University’s Department of Psychiatry, said: “The results are extraordinarily good. We were confident the treatment would prove effective, but the outcomes exceeded our expectations.
“Over three-quarters of the participants receiving the VR treatments showed at least a halving of their fear of heights. Our study demonstrates that virtual reality can be an extremely powerful means to deliver psychological therapy.
“We know that the most effective treatments are active: patients go into the situations they find difficult and practise more helpful ways of thinking and behaving. This is often impractical in face-to-face therapy, but easily done in VR.”
The results are reported in the latest edition of The Lancet Psychiatry journal.
On average, the participants had lived with a fear of heights for 30 years. Before the treatment they were tested to see if they met the criteria for a genuine fear of heights, or acrophobia.
Height experiences began with easier challenges, such as a safety barrier slowly lowering no more than five floors up. As participants became more comfortable with these, they were allowed to be more daring.
Prof Freeman said: “When VR is done properly, the experience triggers the same psychological and physiological reactions as real-life situations. And that means that what people learn from the VR therapy can help them in the real world.”
Participants were enthusiastic about the treatment.
One, Sarah, said: “What I’m noticing is that in day-to-day life I’m much less averse to edges, and steps, and heights … I feel as if I’m making enormous progress.”
Another, Nico, said: “It’s absolutely brilliant … I found myself even after the third floor, fourth floor, going up, feeling nervous, anxious about what’s about to happen next. It definitely pushed the limits in terms of what I thought I would be able to achieve, and then got me to go past that.”
The trial opened up the “exciting” prospect of using virtual reality to tackle other problems such as depression, psychosis and addictions, said Prof Freeman.
He added: “Rigorous testing will be vital, but it feels as though we may be looking at a big part of the future of mental health treatments.”
Dr Mark Salter, from the Royal College of Psychiatrists, said: “We fully support innovative research into the use of information technologies to treat mental illness.
“There are, however, limitations to the study that should be considered before this treatment can be provided as part of routine health care.
“For example, there is no long-term follow up on patients who have received this treatment.
“While the main advantage of this treatment is that it’s cheap, we need to be very cautious before considering machine-based intelligence as an appropriate, easily affordable ‘stand in’ for skilful, well-resourced and empathic health care professionals.”





